

I have always enjoyed having medical students in my office as I like teaching. This week, I had a pleasant 4th year medical student, Andrea. The first day Andrea showed up to my office, I handed her a New England Journal of Medicine (NEJM) article about statin drugs.[i] This is an important article that gave statin drugs the indication to use in a healthy population. I asked her to explain how the authors of the article came to their conclusions and I requested that she do her own statistical analysis and report back to me. When I reviewed the article with Andrea I showed her a different way to look at and dissect the article. Specifically, I pointed out how the conclusions in the article are not supported by the data in the paper. I performed a statistical analysis with Andrea showing her that the article’s data revealed that the drug failed nearly 99% who took it even though the main stream media ridiculously reported a 50% improvement in cardiovascular outcomes. In my book, The Statin Disaster, I discuss the failure of statins for the vast majority who takes them.
For years I have used this article for teaching purposes as it shows how the Big Pharma Cartel makes statin drugs appear to be beneficial when they are not. The next day, I handed Andrea another NEJM article[ii] and told her we would do the same thing. My goal is to teach Andrea and other medical students how to properly analyze a study and come to their own conclusions about whether a drug or therapy is beneficial.
The second article was about Repatha. Repatha is a new cholesterol-lowering medication that works differently from statins. It is part of an expensive class of medications that currently costs about $14,000 per year. When Repatha first came out I predicted that this class of drugs would (similarly to statins) fail and, furthermore, cause too many adverse effects.
When we reviewed the article, we concluded Repatha was not very effective as it failed to help nearly 98% who took it. As we were about to finish our discussion, I said let’s look at the adverse effects from this drug.
I flipped the page to find Table 3:
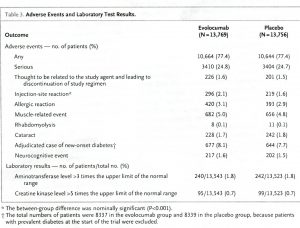
This was the first time I had looked at Table 3 even though I had read the article many times. I commented to Andrea, “Look at the adverse event numbers and look at the serious adverse event numbers.” (This information appears in the first two rows above.)
Since the Chart is difficult to see, here’s what is in the first two rows: Adverse side effects were encountered by 77.4% of those treated with both Repatha and the placebo.
As for serious side effects, 24.8% of the Repatha group and 24.7% of the placebo group suffered a serious adverse effect.
We were both stunned. How could a therapy have such a high rate of adverse effects, especially serious adverse effects? And, how could a placebo have such a high rate of adverse and serious adverse events? (One question that immediately comes to mind is what the heck is in the placebo? That will be coming soon.)
Next, I looked up what the authors classified as adverse events and serious adverse effects. [iii] “An adverse event is defined as any untoward medical occurrence in a clinical trial subject.”
A serious adverse event was defined by the following: “A serious adverse event is defined as an adverse event that meets at least one of the following serious criteria:”
- fatal
- life threatening (places the subject at immediate risk of death)
- requires in-patient hospitalization or prolongation of existing hospitalization
- results in persistent or significant disability/incapacity
- congenital anomaly/birth defect
- other medically important serious event
So, nearly one in four who either took the drug Repatha or a placebo suffered a serious adverse event that includes all the conditions in the bullet points above.
Who would ever take a drug (or a placebo) that is associated with that many serious adverse events?
And, what is in the placebo that is causing so many problems? I thought a placebo was defined as a substance that has no therapeutic effect and is used as a control when testing a drug in order to ascertain if there are any adverse effects from the drug.
But, what do I know?
In fact, this study should have never been published since it did not contain a true placebo—an inert substance that causes no physiologic response. This study was rigged by Big Pharma in order to minimize the side effects from Repatha. Since the side effect profile between the treatment (Repatha) group and the “placebo” group were similar, the authors concluded, “There was no significant difference between the study groups with regard to adverse events…” Based on my findings, I will be calling for the article to be retracted. However, I will not be holding my breath.
Finding out what was in the placebo in the Repatha study was not fun. It was irritating as it was not reported in the original article. The article refers to a Supplemental Appendix for further information. Finding the index and going through it took an inordinate amount of time. More irritations.
However, find it I did on page 49 out of 574 mind-numbing, soul-crushing pages.[iv] The placebo was described here: “Respective placebo will be presented in an identical prefilled AI/Pen containing a 1.0 mL deliverable volume of 1.1% (w/v) sodium carboxymethylcellulose, 250 mM proline, 10 mM acetate, and 0.01% (w/v) polysorbate 20, pH 5.0 or in an identical Personal Injector containing a 3.5 mL deliverable volume of 0.7% (w/v) sodium carboxymethylcellulose, 250 mM proline, 10 mM acetate, and 0.01% (w/v) polysorbate 20, pH 5.0.”
The Repatha drug part of the study (the treatment group) was described as: “Each sterile vial is filled with a 1-mL deliverable volume of 70 mg/mL AMG 145 formulated with 10 mM sodium acetate, 9% (w/v) sucrose, 0.004% (w/v) polysorbate 20, pH 5.2.”
So, what could be causing all those serious adverse effects? It must be something in both the placebo and the Repatha groups. I would put my money on polysorbate as it is found in both groups. It is a toxic substance that has no place in any medicine. Polysorbate is also used in vaccines in the form of Polysorbate 80. The difference between polysorbate 20 and 80 refers to the size of the fatty acid chain. Polysorbate 80, found in many vaccines, is more soluble in lipids than polysorbate 20. Both are widely used in medicine as an emulsifier or defoamer to help the drug disperse.
For polysorbate 20, the Material Safety Data Sheet (MSDS) states, “The toxicological effects of Polysorbate 20 have not been thoroughly studied.”[v] Furthermore, Polysorbate 20 has been investigated as a tumorigenic (promotes tumors) and reproductive effector (adverse effect of a harmful chemical that interferes with the reproductive organs of an organisms). In Section 2 of the MSDS for polysorbate 20 it states for target organs, “No data available.” Later in this section, in regard to signs and symptoms of exposure to Polysorbate 20 the MSDS states, “To the best of our knowledge, the toxicological properties have not been thoroughly investigated.” Under medical conditions generally aggravated by exposure it states, “No data available.” For personal protection exposure: “No data available.” Toxicological information: “The toxicological effects of this product have not been thoroughly studied.”[vi]
Gee, that sounds like a product that I would like injected into me. (I said that with strong sarcasm.)
Repatha should be avoided. In fact, it should be pulled from the market. If your doctor prescribes Repatha ask him/her to explain the 25% serious adverse effects associated with it. Please let me know what you hear.
In part II of this article, I will describe the toxicity of polysorbate 80, which is similar to polysorbate 20. Polysorbate 80 is found in many vaccines.
~Dr B
[i] https://www.nejm.org/doi/full/10.1056/NEJMoa0807646
[ii] https://www.nejm.org/doi/full/10.1056/NEJMoa1615664
[iii] https://www.nejm.org/doi/suppl/10.1056/NEJMoa1615664/suppl_file/nejmoa1615664_protocol.pdf
[iv] https://www.nejm.org/doi/suppl/10.1056/NEJMoa1615664/suppl_file/nejmoa1615664_protocol.pdf
[v] https://www.caymanchem.com/msdss/583151m.pdf
[vi] https://www.caymanchem.com/msdss/583151m.pdf
My boyfriend was prescribed Praluent after refusing statins (on my insistence). All of his cholesterol/triglyceride values are currently below 300, but his docs still want them lower.
Praluent (which has not yet been filled) seems to be similar to the Repatha. Are the medical research results similar? Might this have a 25% rate of serious adverse reactions too? How do I find out?
Karen,
Praluent works the same way Repatha works. It is an unnecessary drug that should not be on the market.
DrB
Dr B, the below CDC website states that mercury in the Measles vaccine, Thimerosal, was removed from the vaccine in 2001. Is this a lie?
https://www.cdc.gov/vaccinesafety/concerns/thimerosal/index.html
Aubrey,
Mercury is not and was not ever in a live virus vaccine.
Mercury was removed from many vaccines, but still is present in others.
DrB
Does homozygous familial hypercholesterolaemia (HoFH) need to be ‘treated’ ? – and is Repatha the appropriate medication?
I shudder to think what the Australian Pharmaceutical Benefits Scheme is forking out on this ‘blockbuster’…
Janet,
With FH, there is a slight increase in death due to heart attacks before the age of 50. After the age of 50, FH patients live longer than those without FH. Most people with FH need no treatment for it.
DrB
This response is so irresponsible. People with Homozygous Familial Hypercholesterolemia absolutely need early treatment to lower their LDL and that will often take multiple medications and even LDL apheresis. Children with HoFH can die of heart attacks without treatment, but there are treatments available and people are now living longer thanks to these treatments. People with Heterozygous FH also need treatment to lower their LDL cholesterol. A recent article cited a 16 year life expectancy reduction for undiagnosed FH. Early diagnosis and treatment for FH can help people with FH live longer, healthier lives. http://www.theFHFoundation.org for more information and to find a doctor who understands FH diagnosis and treatment.
Maybe Cat, don’t quote a money-making foundation to back up your point of view. Other studies clearly show FH need not be treated for LDL reduction. Look more closely at clotting factors and hyperinsulinemia. For your reference, you can start here: cholesterolcode com/cholesterolscience-show-with-dr-david-diamond/
Amazing, the way that Big-pharma can get away with COLD-BLOODED MURDER, isn’t it !!! ? Just call poison and dangerous chemicals by some fancy, high-falootin scientific name, and, there you go !!!
This is the second instance I’m aware of regarding pharmaceutical companies doctoring the placebo, Gardasil being the 1st. As this practice has been publicized, they have started pushing back by stating that the purpose of the studies is to determine the efficacy of the primary components, and, as such, they want to limit the differences between the drug and the placebo to the primary component(s). This is exactly how you would design a study, however, if you wanted to ‘disappear’ the horrible effects of the stabilizers, adjuvants, preservatives, etc.
I’m guessing that a bit of research will show that this is becoming standard practice. It is also medical malpractice, in my opinion.
I leave you with a quote from Marcia Angell, MD., editor of the New England Journal of Medicine for over 2 decades:
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine.”
I know 1st hand of statins, I almost died many times, still suffer now 2000-2007 –lost all motor function for 330-45 min. pain,you name it..muscle weakness still after lost of motor function. I could see and hear only, tried to yell , hardly made a sound, was at work and no one new what had happened. when I came to went to hospital, we cant find nothing… its fraud on the people, I lost my money,jobs, health, had to sell my land. to stay alive.
Very interesting info. I have never been on statins (age 69) and never will I take them. I’d rather take a few vitamin C pills during the day. As far as the MSDS goes, discovering that there is no data for questionable substances is a giant red flag in my view. I have heard where some medical professionals want to start children at about age 10 on statins. We are heading toward medical system Armageddon as we are being poisoned by more and more drugs…directly or in our foods. It just seems to me that since most drugs cause some kind of reaction or adverse side effects, that they are not suitable for use. The foods I eat and the supplements I take do not cause any side effects unless they are tainted or rotten. I think that most drug studies are tainted and never see the light of day. The ones that do often cannot be trusted because Big Pharma has direct influence on many studies.
Many of my colleagues who have been facile enough to fall for the lipid hypothesis in the first place will doubtless see this new wave as a breakthrough bandwagon to jump on. Patients on the other hand are becoming more skeptical. What could be more preposterous than Mab’s to lower LDL ? Thanks for your always informative blog.
THANKS for keeping us informed.
Dr. Brownstein,
As you know, after several years of being on various Statins at my Dr’s insistence, these drugs made me feel terrible with debilitating muscle pain and nerve issues, not to mention fatigue and other symptoms. As if that wasn’t enough, I still had a widow-maker heart attack! My cardiologist then also picked up the mantle from my regular doctor and insisted that I continue on the Statins. Last year (about 1 yr post heart attack) I had enough. I was feeling so bad that I came to see you. I immediately stopped taking Statins and within a few short weeks, I felt significant improvement and today I feel even better. Yes, my cholesterol is still high, I am working on that, but feeling better allows me to focus on getting more exercise and eating better. My cardiologist is definitely not happy and is insisting that I get back on medicine. I told him I was on Statins for 8 years, feeling terrible the whole time and I still had a heart attack. That produced a stunned look! So now, he is insisting I go on Repatha because it is perfect for people who can’t tolerate Statins. That is not going to happen, especially based on their own research results and I look forward to my next appointment when he brings it up again and I ask him to tell me about the 25% adverse effects! Thanks for the information and the critical questions required to properly participate in dealing with health issues and treatments that are being pushed on us under false advertising.
Scott,
Please let me know what the response is to the serious adverse effects associated with Repatha.
DrB
My doctor’s have been recommending statin drugs for me since I was 50. My LDL cholesterol levels used to be around 240, but I have never agreed to take them. In my recent physical, my LDL is up to 278, and my doctor is strongly recommending a statin drug. I am now 65 and all my other heart and health factors are fine – great blood pressure, no sign of heart issues (I had a full series of tests done including stress test), etc. So, I am feeling that I will NOT take the drug and rather I will work on exercising more, changing my diet, and losing some weight. What do you think? How high is too high for LDL?
After my doctor tried to kill me with pravachol (extremely sore and weak muscles); and then zetia (severe widespread pain that sent me to the ER)- he tried to presribe Praluent (biologic injectible similar to Repatha). I flat out refused! I may be shopping for another doctor soon.
Thank you, Dr. B for making information available and making it easy to understand for those of us who don’t have PhD’s.
I have read that many of the Vitamin K injections given to new-born babies have polysorbate 80. I understand that there is a Vitamin K formulation that doesn’t have polysorbate 80, but instead has Benzyl Alcohol which may be even more toxic.
The amount of quality research on this subject of Vitamin K shots is miniscule, and I have not seen any convincing scientific proof that the benefits of this common medical intervention outweigh the harms. It seems that the precautionary principle is being misused to justify this practice on the basis that it might prevent internal bleeding in the newborn child.
I think that the precautionary principle would dictate not injecting this toxic, poorly studied stuff.
Repatha is a PCSK9 inhibitor. Your article misses some important understanding and knowledge. I am a holistic doctor with advanced nutrition degrees. This “medication” (its really a mono-clonal antibody would only be beneficial in a very small subset of the population with that particular mutation. However even though I prefer natural remedies there is a argument that this would do well for that subset. Medical Genomics is in a race with Nutragenomics. In this case I think you oversimplify. I would be happy to discuss further.
John,
The purpose of the article was to call out a drug (and a fake placebo) that causes serious adverse effects in one in four who take it. I don’t think an advanced nutrition degree is needed here.
DrB
John, I assumed (incorrectly) that the drug in the study was only used on people in that specific subset that you mentioned. And that these were the results thereof. I now see how wrong my thinking is. I’ve never actually read a study. Does it state in what cases (and/or subsets, tests to show proof of a need) to use their drug?
Dr Brownstein, my first thought was about the plecebo….if the drug (something) had the same nasty effects as a placebo (a nothing) then I’ll stick with doing “nothing” and not take the drug!
Lisa,
The drug is being used more and more, not just in a subset of patients. Patients with elevated cholesterol levels, already treated with a medication, was eligible. The “subset” argument is ridiculous. That was not the focus of the post nor is it relevant to how the drug is being promoted and utilized.
DrB
Polysorbate’s in a lot of supplements, too. And in make up as well. Reading labels is wearisome, but at least with supplements, et al, there’s a label to read.
Bette,
It is. However, injecting it may be more toxic. Of course, it would be nice if FDA and the Powers-That-Be studied it before allowing it in so many consumer items, especially injectables.
DrB
A few years ago I read an article, I believe it may have been by Dr Brownstein, on polysorbate 80. I had bought a large bottle of vitamin C from one of the buy quantity stores without my reading glasses so I couldn’t make out all of the fine print ingredients. They were large 500mg orange flavored tablets. I took a few and then read the fine print. Polysorbate 80 was one of the ingredients. The entire bottle went in the trash. I was flabbergasted by the toxic ingredients that are routinely added to pharmeceuticals. You definitely have to read the fine print and this study illustrates the mischief that is being committed unnecessarily. Vaccines is another subject that I could write books about in regard to the lack of independent research and the overt attempts by both big pharma and the CDC to discredit any studies that find any dangers involved with any of the ingredients. Specifically the Italian study on 44 different vaccines administered in Europe and the confiscation of all equipment, computers and documents related to the study findings a month after publication of the results.
I commend Dr Brownstein for his courage in exposing the truth about the methods used to blindside patients and a lot of doctors who take the CDC at its word without supporting research findings. It appears to me that adverse vaccine reactions were by far less common pre 1988 when Congress granted blanket immunity to big pharma for adverse events related to vaccines. That date stands out as the point at which adjuvants began being added to vaccines to enhance immune responses. It appears that enhanced immune responses were not the only result. Thanks again Dr B for looking after both sides of these medications. You are to be commended.
My father died within 6 months of using Repatha
He was continually going to the ER and ending up by spending days and days in hospital with not getting any better
From the first injection he had lots of bruising and then trouble breathing and then got a cough
By the time he decided to stop using it …it was too late
Ros,
Sorry to hear about your father.
DrB